
 By: Brigid Martz Smith -
By: Brigid Martz Smith -
Women who have a high risk of breast or ovarian cancer face a number of looming decisions; from whether or not to undergo prophylactic surgery, to electing increased surveillance, to taking risk-lowering medication. Interwoven with these decisions is the implication each will have on fertility. The next chapter in Oncofertility Communication: Sharing Information and Building Relationships across Disciplines delves into the topics discussed during a high-risk consultation and provides case examples to illustrate the role of effective communication of fertility preservation options.
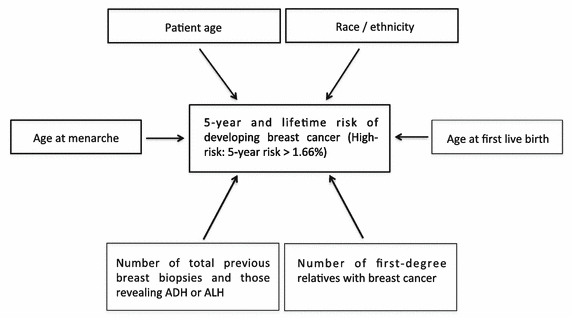
Chapter 5: Fertility Communication and High-Risk Patients begins with the authors, Dr. Jacqueline Jeruss and Natalia C. Llarena, defining high-risk patients. High-risk patients, are women with a genetic predisposition to breast or ovarian cancer (BRCA1 and BRCA2) who will develop malignancies at a higher rate and younger age than a general population. Due to this, preventative therapy is indicated before menopause. Female carriers of BRCA1 and BRCA2 mutations have a 45-65% lifetime risk of developing breast cancer and an 11-39% lifetime risk of developing ovarian cancer. Women without a known genetic mutation, but who have a strong family history of breast or ovarian cancer, are also at an increased risk. Their risk can be better calculated through risk assessment tools such as the Gail model. The Gail model estimates the patient’s 5-year and lifetime risk of developing breast cancer by taking in account the patient’s age, age at menarche, age at first birth or nulliparity, family history in primary relatives, race/ethnicity, number of previous breast biopsies, and number of breast biopsies that yielded atypical cells. Both the Gail model calculation and information relating to known genetic mutations allows clinicians to accurately communicate risk to their patients and present risk-reducing treatment options.
 Such risk-reducing options include prophylactic bilateral salpingo-oophrectomy (BSO) and prophylactic mastectomy. These are recommended to be done after age 35 (but before menopause) or as soon as the patient is finished having children. However, women with a strong family history of early-onset cancer should consider pursuing surgical intervention at an earlier age. If surgical intervention is not elected at the time, patients are recommended to undergo antiestrogen treatment with tamoxifen which offers considerable therapeutic benefit. Unfortunately, tamoxifen is a teratogen and pregnancy should be avoided during the duration of treatment; typically 5-10 years. Each of these risk-reducing strategies should be comprehensively discussed during the patient’s initial high-risk consultation after reviewing the patient’s medical history, and childbearing and lactation history. Many clinicians have indicated that basic questions, such as “Were you thinking about having a child?” or “Were you planning on having more children?” can help initiate the conversation about fertility implications.
Such risk-reducing options include prophylactic bilateral salpingo-oophrectomy (BSO) and prophylactic mastectomy. These are recommended to be done after age 35 (but before menopause) or as soon as the patient is finished having children. However, women with a strong family history of early-onset cancer should consider pursuing surgical intervention at an earlier age. If surgical intervention is not elected at the time, patients are recommended to undergo antiestrogen treatment with tamoxifen which offers considerable therapeutic benefit. Unfortunately, tamoxifen is a teratogen and pregnancy should be avoided during the duration of treatment; typically 5-10 years. Each of these risk-reducing strategies should be comprehensively discussed during the patient’s initial high-risk consultation after reviewing the patient’s medical history, and childbearing and lactation history. Many clinicians have indicated that basic questions, such as “Were you thinking about having a child?” or “Were you planning on having more children?” can help initiate the conversation about fertility implications.
Fertility concerns are a major factor for high-risk patients when selecting deciding on cancer risk management. Fertility preservation options have the potential to influence patients’ selection for risk-reducing strategies and when to pursue risk reduction. As such, it is critical for clinicians to educate patients on their options for fertility preservation early in the process of cancer risk management. The chapter continues on to present two case studies: one where the female patient declined fertility preservation and the other where the female patient elected to undergo fertility preservation. High-risk patients face complex decisions about how to prioritize preventative treatment, childbearing, and breastfeeding. Physicians are faced with the ongoing challenge of ensuring that high-risk patients understand their cancer risk and are adequately informed of their options for preventative treatment and fertility preservation.
Review Chapter 5 of Oncofertility Communication today and review additional case studies through the Oncofertility Consortium’s Virtual Grand Rounds.