
Galactosemia
| Incidence | Galactosemia affects between 1:16,000[1] to 1:60,000[2] individuals. |
| Natural History | 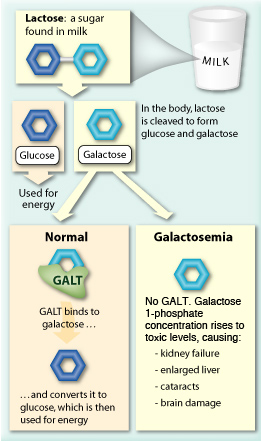 Classic Galactosemia (ORPHA79239) is an autosomal recessive inherited metabolic disorder caused by deficient activity of galactose-1-phosphate uridyl transferase (GALT), as a result of mutations in the GALT gene. GALT is the second of three enzymes in the Leloir pathway- the main pathway of galactose metabolism. Classic Galactosemia (ORPHA79239) is an autosomal recessive inherited metabolic disorder caused by deficient activity of galactose-1-phosphate uridyl transferase (GALT), as a result of mutations in the GALT gene. GALT is the second of three enzymes in the Leloir pathway- the main pathway of galactose metabolism.
Galactose is needed for energy metabolism and glycosylation of complex molecules. It can be derived two ways: either from exogenous (dietary) sources like lactose from dairy products, or by endogenous production. A deficiency of GALT enzyme leads to accumulation of galactose and its metabolites in the body and results in secondary glycosylation abnormalities[3]. Almost all infants born in the US with Galactosemia are diagnosed through state newborn screening programs. |
| Disease Presentation | 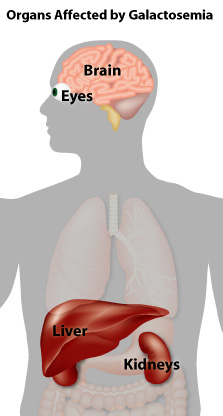 The symptoms of Galactosemia present during the first few weeks of life with signs of liver and renal disease, cataracts, and an Escherichia coli sepsis. A galactose-restricted diet resolves the early signs of Galactosemia, but it cannot prevent development of later-onset complications, such as: The symptoms of Galactosemia present during the first few weeks of life with signs of liver and renal disease, cataracts, and an Escherichia coli sepsis. A galactose-restricted diet resolves the early signs of Galactosemia, but it cannot prevent development of later-onset complications, such as:
|
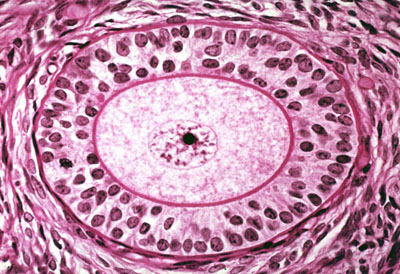
| Effect on Fertility | Almost every female with classic Galactosemia develops primary ovarian insufficiency (POI) as a diet-independent complication of the disease[4]. POI can vary from subfertility, to early development of irregular menstrual cycles and infertility, to primary amenorrhea and absence of spontaneous puberty. The mechanisms causing ovarian dysfunction are unknown. Postulated mechanisms of ovarian dysfunction include:
In general, POI is either caused by formation of a smaller primordial follicle pool or more rapid loss of primordial follicles[3]. Evidence of both has been seen in individuals with Galactosemia. Neonates have been reported with morphologically normal ovaries with abundant ooctyes and normal folliculogenesis[5,6]. Adolescents (16-17 years of age) have histological findings showing strongly reduced number of follicles, varying from far fewer follicles than expected for age[7] to almost complete absence[8,9]. Additionally, patients age 9-21 years were found by ultrasound or laparoscopy/laparotomy to have hyoplastic[9,10] or streak ovaries[8]. It is possible that a normal complement of primordial follicles forms, but undergoes atresia more rapidly and that the ovaries can be severely damaged in girls at very young prepubertal ages[3]. |
| Fertility Preservation | Fertility preservation options should be presented to females with classic Galactosemia as early as possible. Three fertility preservation procedures are currently offered to girls and women in need of fertility preservation, including:
Ovarian Tissue Cryopreservation Embryo and oocyte cryopreservation are, in theory, the best options for these patients. However, both techniques require ovarian stimulation. Gubbels et al. (2013) conducted ovarian stimulation in 15 classic Galactosemia patients, age 15-36 years, and demonstrated poor estradiol production in all patients except for one[11]. Therefore, fertility preservation in older, postpubertal classic Galactosemia patients is likely to be unsuccessful as the ovarian reserve may be poor. Considering the poor estradiol production and rapid follicle pool decline in classic Galactosemia, fertility preservation in these patients may need to take place during infancy or early childhood, seriously limiting fertility preservation options. Techniques requiring ovarian stimulation, such as embryo and oocyte cryopreservation, are not suitable for prepubertal girls because of absence of maturation of the hypothalamic-hypophyseal-ovarian axis, leaving cryopreservation of ovarian tissue the only available technique for this age group. Females with classic Galactosemia may wish to pursue other options, including adoption or donor oocytes to achieve pregnancy. Additionally, mothers of girls with classic Galactosemia frequently propose to donate oocytes for their daughters. It may be necessary to cryopreserve the mother’s oocytes for the future if the patient is not ready for children at the time of donation[3].
Spontaneous Pregnancy Spontaneous pregnancies do occur in classic Galactosemia, demonstrating that conception is possible in some patients[3]. It is important to educate patients about the occurrence of spontaneous pregnancies, allow them to try to conceive spontaneously, and avoid unplanned pregnancies. Gubbels et al. (2008) had a cohort of 22 patients with classic Galactosemia and POI. 9 patients in the cohort tried to conceive and 4 succeeded, resulting in a 44% success rate. The small sample size warrants further studies in larger cohorts. Additionally, it is important to note that most of the women who became pregnant spontaneously had gone through normal puberty and reached menarche spontaneously, indicating that these may be predictive factors for an increased chance of spontaneous conception[12]. |
| Expert Opinion | van Erven et al. (2013) has published the following recommendations based on expert opinion regarding fertility preservation in female classic galactosemia patients:
|

References
[1]Coss, K., Doran, P., Owoeye, C., Codd, M., Hamid, N., Mayne, P., . . . Treacy, E. (2012). Classical Galactosaemia in Ireland: incidence, complications and outcomes of treatment. J Inherit Metab Dis, 36, 21-27.
[2]Berry, G., & Elsas, L. (2011). Introduction to the Maastricht workshop: lessons from the past and new directions in galactosemia. J Inherit Metab Dis, 34, 249-255.
[3]van Erven, B., Gubbels, C., van Golde, R., Dunselman, G., Derhaag, J., de Wert, G., . . . Rubio-Gozalbo, M. (2013). Fertility preservation in female classic galactosemia patients. Orphanet J Rare Dis, 8, 107.
[4]Fridovich-Keil, J., Gubbels, C., Spencer, J., Sanders, R., Land, J., & Rubio-Gozalbo, E. (2011). Ovarian function in girls and women with GALT-deficiency galactosemia. J Inherit Metab Dis, 34, 357-366.
[5]Levy, H. (1996). Reproductive effects of maternal metabolic disorders: implications for pediatrics and obstetrics. Turk J Pediatr, 38(335-344).
[6]Levy, H., Driscoll, S., Porensky, R., & Wender, D. (1984). Ovarian failure in galactosemia. N Engl J Med, 310, 50.
[7]Rubio-Gozalbo, M., Gubbels, C., Bakker, J., Menheere, P., Wodzig, W., & Land, J. (2010). Gonadal function in male and female patients with classic galactosemia. Hum Reprod Update, 16, 177-188.
[8]Morrow, R., Atkinson, A., Carson, D., Carson, N., Sloan, J., & Traub, A. (1985). Ovarian failure in a young woman with galactosaemia. Ulster Med J, 54, 218-220.
[9]Robinson, A., Dockeray, C., Cullen, M., & Sweeney, E. (1984). Hypergonadotrophic hypogonadism in classical galactosemia: evidence for defective oogenesis Case report. Br J Obstet Gynaecol, 91, 199-200.
[10]Sauer, M., Kaufman, F., Paulson, R., & Lobo, R. (1991). Pregnancy after oocyte donation to a woman with ovarian failure and classical galactosemia. Fertil Steril, 55, 1197-1199.
[11]Gubbels, C., Land, J., Evers, J., Bierau, J., Menheere, P., Robben, S., & Rubio-Gozalbo, M. (2013). Primary ovarian insufficiency in classic galactosemia: role of FSH dysfunction and timing of the lesion. J Inherit Metab Dis, 36, 29-34.
[12]Gubbels, C., Land, J., & Rubio-Gozalbo, M. (2008). Fertility and impact of pregnancies on the mother and child in classic galactosemia. Obstet Gynecol Surv, 63, 334-343.
About the Author
Allison Goetsch, MS, CGC is a pediatric genetic counselor at Ann and Robert H. Lurie Children’s Hospital of Chicago and a member of the Oncofertility Consortium administrative core team. She completed her graduate thesis with Dr. Teresa K. Woodruff researching oncofertility and hereditary breast and ovarian cancer (HBOC) syndrome. Allison’s primary goals are to increase fertility preservation awareness and education for both health care providers and patients regarding malignant and non-malignant diseases (and/or treatments) which threaten fertility.
This page was last updated February 6th, 2016.